|
|
|
|
|
|
||
|
|
||
|
|
||
|
CCSVI, Chronic Cerebro-Spinal Venous Insufficiency for MS PatientsInternational center for cardiovascular diseases started two years ago with studying and evaluating pathological process of head and neck vein system, particullary in patiens with MS disease.
MC MEDICOR developed in last ten years with experienced team and modern technology the best treatment of cardiovascular diseases in European region. The vision of our work is not only to create the best medical practice, but also to implant research work as a tradition with which we follow the idea of our great teacher, Prof. Dr. Renee Favaloro: from basic research to clinical practice. Due to the reason that CCSVI idea for MS is new and exciting development, we decided to organize exceptional diagnostic procedures and therapy to help patients all over the world. From the beginning we were aware that we need to create a special team of scientists and co-workers who will join the knowledge in the field of neurology, cardiology, invasive diagnostic procedures and vascular therapies, particulary due to the fact in spite of vascular pathology, multiple sclerosis is neurological disease. Exceptional interventional vascular radiologist Assist. Prof. Dr. Zoran Milosevic, experienced clinical neurologist Msc. Dr. Marjetka Clemenz and experienced cardiologist and also researcher in the field of vascular pathology, Prof. Dr. Metka Zorc, performed as a team treatment of MS patients.
This
special place � MC MEDICOR Izola gave us the opportunity to create complete
diagnostic and treatment of MS patients with promising results and
exact neurological evaluations.
We are responsible to contact and to
respond immediately. Our secretary Ms. Ljiljana Popovic will give everybody
additional information. Information about the procedure and about the principles of our work Multiple sclerosis (MS) is a chronic acquired autoimmune disease of unknown origin manifested by different symptoms and signs. At the same time a damage of the protective coating around the nerves � myelin and underlying nerve fibre occur. The lesions through CNS are disseminated in space and time. The first symptoms appear often as sensory disturbance � frequent or continuing tingling and numbness. Other symptoms include muscular weakness � paresis, poor coordination and balance, rigidity in particular muscle group � spasticity. Bladder, bowel and sexual function rarely occur in the early stages of disease. Fatigue is another common non-specific symptom of the disease. Optic neuritis is also common the first manifestation of MS. The initial manifestation is so called clinically isolated syndrome presenting as subacute dysfunction of the optic nerve, brain or spinal cord. Relapsing-remitting course of disease occurs in 85% of the patients. Only a small number of patients (10%) develop slowly progressive disability without relapses and remissions. The disease modifying drugs suppress inflammatory phase of MS. Oral drugs are expecting soon. The topic of chronic cerebrospinal venous insufficiency (CCSVI) has generated the great interest. After the first angioplastic procedure published by Dr. Paolo Zamboni many studies started. In MS Centre Medicor Izola balloon dilatation of the jugular in azygous veins is performed. Our results are encouraging. THE PROTOCOL FOR DIAGNOSTIC PROCEDURES (outpatient department)
1. Review of
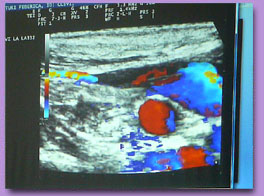
medical documentation with history of the disease and plan for the 2. Neurological evaluation: clinical examination, assessment of EDSS and course of multiple sclerosis (RR MS, SP MS, PP MS), duration of the disease, information about therapy with imunomodulatory drugs, bladder dysfunction, 25 FTW - walking ability, nine hole peg test, brief fatigue inventory test, quality of life according VAS. 3. Cardiological investigation: clinical status, ECG, Heart Ultrasound, Ultrasound of carotid arteries. 4. Specific investigations: ultrasound of jugular veins. THE PROTOCOL FOR DIAGNOSTIC AND TREATMENT (in hospital) 1. Admission in the hospital with all the data form outpatient department. 2. Pre treatment Therapy: Aspirin 100 mg, Plavix 75 mg. 3. Investigation: venography of jugular veins and vena azigos. 4. Treatment: PTA of stenosis in jugular veins (right and left) and vena azigos (diagnosed directly with venography). 5. Review of neurological results the next day. 6. The therapy for discharge: Aspirin 100 mg � 6 months, Plavix 75 mg � 3 months, Detralex (Diosminum � Hesperidinum) � 6 months. 7. Instructions for physiotherapy and life management with continuous controls every month (neurological status and cardiological investigations and therapy if necessary). 8. Control ultrasound investigation of jugular veins after 6 months.
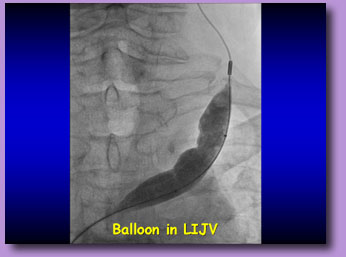
TECHNIQUE OF THE PROCEDURE
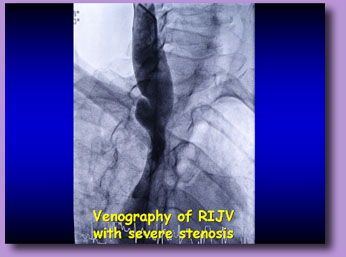
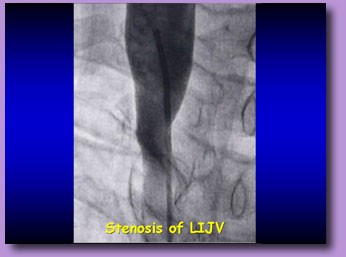
The catheter is then placed in succession into the AZV and both IJVs. The catheter is positioned in the AZV at the junction with the hemiazygos vein. Contrast venography is done at 3 mL/s for a total volume of 10 mL to look for reflux, followed by a second, fuller injection at 8 to 10 mL/s for a total volume of 20 to 30 mL to delineate all the anatomy. The AZV and its tributaries are imaged to include the chest and abdomen. Some physicians measure pressures, but I have not found this to be helpful. Any stenosis is treated, as will be described later. The catheter is then withdrawn from the AZV and advanced sequentially into each IJV. Catheterization of the IJV may be challenging because funneled narrowing of stenotic valve leaflets occurs near the origin of the vessel. Two contrast injections are performed: one with a slow injection of 3 mL/s for a total volume of 10 mL and one with a fuller injection of 8 to 10 mL/s for a total volume of 20 mL. Film rates of 3 to 6 frames per second are necessary to get sufficient detail of the valves and to detect ostial narrowing that may become obscured as contrast enters the brachiocephalic veins and overlaps the confluents where stenosis is often located. Any stenosis or other outflow obstructions are treated at this time. Diluted contrast abnormalities (50:50 mixture of saline) is helpful in the IJV evaluation because valve abnormalities and some webs may be obscured by very dense contrast media.
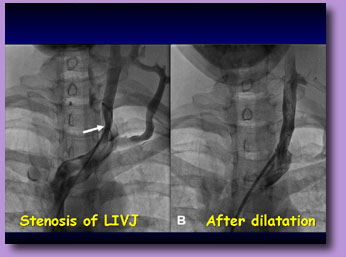
Venographic Finding
Venous Angioplasty
Angioplasty with high-pressure balloons of diameters from 4 mm to 16 mm in 2 cm to 4 cm lengths is performed with venographic control. Inflations to maximum pressures 12 atm to 16 atm for 30 to 60 seconds were used several times. Some of these obstructions are very resistant. Stenting is performed by some investigators for resistant narrowings. However, no reports have been published about their outcomes. I have not used stents in any cases yet.
OUR RESULTS
Click to see patient's impression, two days after venous dilatation ► |
Exact ultrasound investigation Please contact us on the following telephone numbers:
00 386 5 662 55 15
Fax: 00 386 5 662 55 56
|
||||||||||||||
|
Best viewed with |
This site maintained by the Computer Center of the International Center for Cardiovascular Diseases |
||||||||||||||